Pneumocystis jirovecii
Pneumocystis was initially considered a protozoan and was subsequently assigned to the kingdom Fungi based on phylogenetic studies of the rRNA (Edman et al., 1988).
Pneumocystis is included in the phylum Ascomycota, subphylum Taphrinomycotina, and is related to Saccharomyces cerevisiae and Schizosaccharomyces pombe. Despite these similarities, Pneumocystis is considered an “atypical fungus” as it has cholesterol in its cell membrane instead of ergosterol and is difficult to culture (Edman et al., 1988). Initially considered a single species, Pneumocystis carinii, it has since been discovered that different species infect different mammals and the species are both phenotypically and genetically distinct (Sinclair et al., 1991). The human form was renamed Pneumocystis jirovecii and other species-specific forms have been named P. murina in mice, P. carinii and P. wakefieldiae in rats and P. oryctolagi in rabbits (Cushion, 2010).
Pneumocystis jirovecii is ubiquitous and causes P. jirovecii pneumonia (PCP) in patients with T cell deficiencies, including those with HIV infection, solid organ transplant recipients and patients with cancer as well as adults and children with other underlying immunological diseases (Alanio et al., 2016). P. jirovecii is not cultivable in vitro and diagnosis of proven PCP is based on clinical and radiologic criteria and demonstration of P. jirovecii by microscopy.
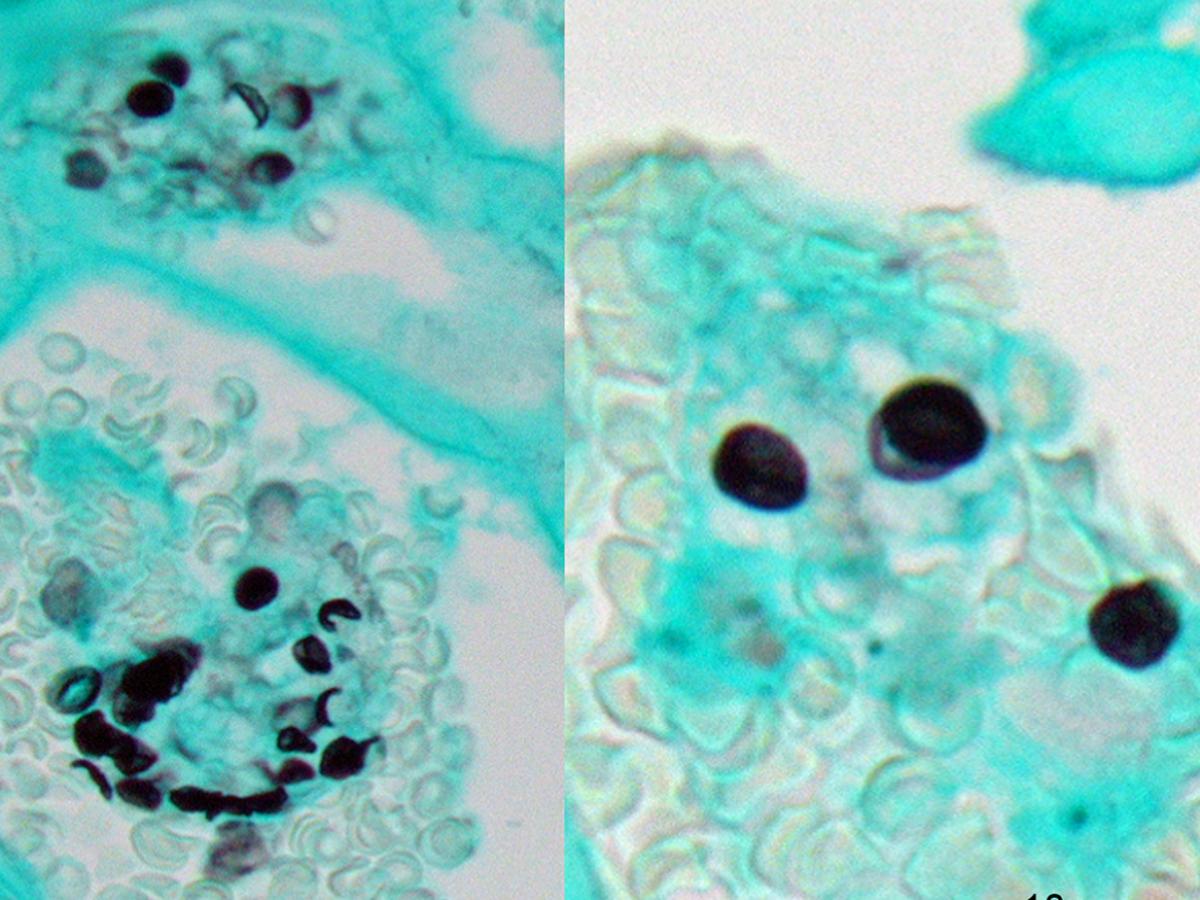
Pneumocystis jirovecii cysts in a Grocott-Gomori’s methenamine silver-stained tissue section from a lung biopsy (Photograph courtesy Yee Khong, Anatomical Pathology, SA Pathology, Adelaide, Australia).
Morphological description: Diagnosis relies on microscopic detection of trophic forms and cysts of P. jirovecii in induced sputum, expectorated sputum and bronchoalveolar lavage fluid or washings. The most commonly used stains, i.e. Giemsa, toluidine blue O, calcofluor white and Grocott-Gomori’s methenamine silver, stain the cyst form only. Cysts are non-budding, 4-8 µm in diameter, round, oval or collapsed crescent in shape, resembling crushed ping pong balls or parentheses facing one another, often found in honeycomb-like clusters (Fig. 78.1). Immunofluorescent staining exhibits superior sensitivity to conventional microscopy detecting both the cyst and trophic forms, which are 10 x more abundant than the cyst forms in clinical specimens (Alanio et al., 2016). Trophozoites are 1-8 µm long, pleomorphic and contain a single nucleus.
Key features: Intracystic bodies resembling parentheses facing one another or crushed ping pong balls often found in honeycomb-like clusters.
Molecular identification: PCR-based assays are more sensitive than microscopic examination for the detection of P. jirovecii, but they cannot distinguish between colonisation and infection. The multi-copy mitochondrial large subunit ribosomal RNA (mtLSU) gene is the most common PCR target, but assays targeting the mitochondrial small subunit RNA (mtSSU) gene, major surface antigen gene, 18S rRNA, ITS, β-tubulin, DHPS and HSP70 genes have also been developed (Lagrou et al., 2021).
References: Edman et al. (1988); Sinclair et al. (1991); Cushion (2010); Alanio et al. (2016); de Hoog et al. (2020); Lagrou et al. (2021).